

What is Uveitis?
Uveitis [u-vee-i-tis] is a term for inflammation of the eye. It can occur in one eye or both eyes and affects the layer of the eye called the uvea [u-vee-uh]. It also can be associated with inflammation of other parts of the eye and last for a short (acute) or a long (chronic) time. Uveitis can be serious and lead to permanent vision loss. That is why it is important to diagnose and treat uveitis as early as possible, ideally before irreversible damage has occurred. Uveitis causes about 30,000 new cases of blindness each year in the United States.
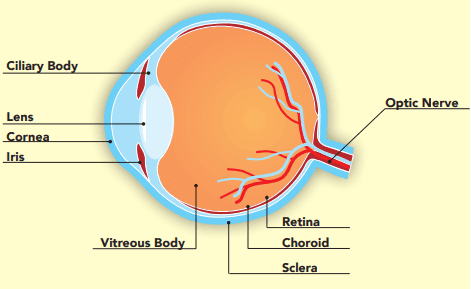
The uvea is a layer of the eye made up of three parts from the front to the back of the eye that helps provide nutrients to the eye.
Choroid [kawr-oid]: The choroid is a middle layer of the back wall of the eye. It holds blood vessels that feed other parts of the eye, especially the retina.
Ciliary [sil-ee-er-ee] body: The ciliary body is a group of muscles and blood vessels that changes the shape of the lens so the eye can focus. It also makes a fluid called aqueous humor. Aqueous humor is a clear, watery fluid that fills and circulates through parts of the front of the eye.
Iris: The iris is the colored part of the front of the eye. It controls light that enters the eye by controlling the size of the eye’s opening (the pupil).
Inflammation of the uvea may be associated with inflammation of other parts of the eye:
Cornea: The clear, curved front of the eye
Sclera [skleer-uh]: The white outer part of the eye
Vitreous [vi-tree-uh s]: A gel-like substance that fills the inside of the eyeball between the lens and the retina
Retina: The inner layer lining the inside back wall of the eye which contains nerve cells that sense color and light and send image information to the brain Optic nerve: It sends information from the eye to the brain
Optic nerve: It sends information from the eye to the brain
What Causes Uveitis?
Uveitis is a form of inflammation of the eye. The cause of uveitis is often unknown in at least one-third of cases. The inflammation could be caused by:
- Eye injury or surgery
- Infection
- Autoimmune diseases or systemic inflammatory disorders that affect the whole body
Causes of Anterior Uveitis
Causes of Anterior Uveitis In more than a third of anterior uveitis cases, the exact cause is unknown but may include:
- Ankylosing spondylitis
- Reactive arthritis
- Psoriatic arthropathy
- Inflammatory bowel disease
- Juvenile idiopathic arthritis (JIA)
- Herpes
- Sarcoidosis
- Fuch’s heterochromic iridocyclitis
- Lupus
- Intraocular lens surgically implanted to replace a cataract lens
- Posner-Schlossman syndrome (PSS)
- Rheumatoid arthritis
- Syphilis
- Tuberculosis (TB)
- Lyme disease
Causes of Intermediate Uveitis
In more than two thirds of all cases of intermediate uveitis, the exact cause is unknown. The remaining third of all cases are thought to be caused by conditions such as:
- Sarcoidosis
- Multiple sclerosis (MS)
- Lyme disease
Causes of Posterior Uveitis
In more than one in ten cases of posterior uveitis the cause is unknown. The following is a list of common causes of posterior uveitis.
- Toxoplasmosis
- Cytomegalovirus retinitis (CMV retinitis)
- Lupus
- Birdshot retinochoroidopathy
- Sarcoidosis
- Acute retinal necrosis
- Epstein-Barr virus (EBV)
- Behcet’s disease
- Syphilis
- Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)
- Serpiginous choroidopathy
Causes of Panuveitis
As with other kinds of uveitis, the cause of panuveitis is often unknown. Other possible causes include:
- Sarcoidosis
- Behcet’s disease
- Lupus
- Syphilis
- Vogt-Koyanagi-Harada syndrome
- Tuberculosis (TB)
- Fungal Retinitis
Causes of Uveitis in Children
Often, the cause of the uveitis is unknown. Juvenile idiopathic arthritis (JIA) is a leading cause of uveitis in children.
- Juvenile idiopathic arthritis (JIA)
- Toxoplasmosis
- Toxocariasis
- Sarcoidosis
- Vogt-Koyanagi-Harada syndrome
- Acute retinal necrosis
- Reactive arthritis
- Lupus
- Behcet’s disease
- Fuch’s heterochromic iridocyclitis
- Chicken pox
Uveitis Symptoms?
Uveitis symptoms may occur quickly in an acute form (lasts less than six weeks) or slowly in a chronic form (lasts longer than six weeks). These symptoms may get worse fast, and also may affect one or both eyes.
The signs and symptoms of uveitis include:
- Eye redness
- Eye pain
- Light sensitivity
- Blurred vision
- Dark, floating spots in your field of vision (floaters)
- Decreased vision
Anyone suffering from the symptoms above should immediately be examined by an eye care professional.
What Increases the Risk for Uveitis?
Uveitis can affect anyone at any age, but it is most commonly seen in working age adults in their fourth decade. There is a higher prevalence in women. As we age, however, we are more likely to get uveitis in both eyes and panuveitis (uveitis that affects all of the uvea). In addition, smoking may increase the risk of getting uveitis.
What are the Types of Uveitis?
Uveitis is often grouped by the part of the uvea it affects. There are four types of uveitis:
- Anterior uveitis
- Intermediate uveitis
- Posterior uveitis
- Panuveitis
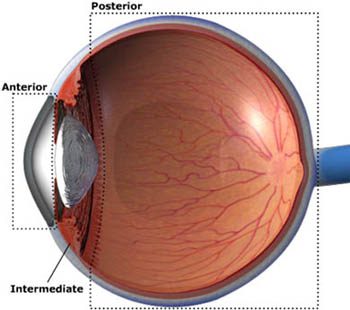
Anterior Uveitis affects the front of the eye. It is often called iritis because it mainly affects the area around the eye’s iris. Anterior uveitis is the most common kind of uveitis in children and adults making up 30–90% of all uveitis. It is usually acute (comes on quickly and lasts for less than six weeks) and is associated with eye pain, blurred vision, light sensitivity and redness. Intermediate Uveitis Intermediate uveitis is inflammation of the ciliary body, the front end of the retina, and the vitreous.
Intermediate Uveitis is the least common type of uveitis affecting young adults, making up only 1–12% of cases. It is also known as cyclitis, pars planitis or vitritis. Symptoms include floaters and blurry vision. It is not usually associated with pain. People with intermediate uveitis are more likely to have chronic inflammation. Chronic uveitis is defined as uveitis lasting longer than six weeks.
Posterior Uveitis is inflammation of the choroid, often involving the retina and optic nerve. and optic nerve. It is also known as choroiditis or retinitis. The optic nerve is the path that carries images from the retina to the brain. It can be seen in 5–30% of uveitis types. Generally it is chronic (long standing – can last weeks to months to years), recurrent (in which a patient goes between inflammation and a healthy eye) and affects both eyes. Posterior uveitis can cause vision loss. This type of uveitis can only be detected during an eye examination.
Panuveitis is when inflammation affects the entire uvea (iris, ciliary body, and choroid). It makes up 1–9% of cases. People with panuveitis may be more likely to experience vision loss. Symptoms include floaters, blurred or loss of vision.
Diagnosis and Treatment
Diagnosis and treatment of uveitis is important. Uveitis can cause permanent damage to the eyes and vision loss that cannot be reversed. Also, uveitis may be caused by another disease or condition that, if left untreated, can lead to serious illness.
Complete eye examination
Anyone who notices signs of eye problems should visit an eye doctor for a complete eye exam. At a complete eye exam, the eye care professional will do a thorough examination of the eyes, using some of the following tests:
Medical history: Since uveitis is often caused by other diseases and conditions, it is important to get a thorough medical history.
Ophthalmoscopy [of-thal-mos-kuh-pee]: The eye doctor will look inside the eyes and check the optic nerve at the back of the eye by putting drops in your eyes to make the pupils bigger (dilate).
Visual acuity: The eye doctor will test the sharpness of your vision.
Visual field: Damage to the optic nerve may cause a loss of side vision (peripheral vision). A visual field test can check your peripheral vision for any changes. Pupils and eye movements: The eye doctor will look at your pupils to check for signs of eye problems and check the movement of the eyes.
Gonioscopy [goh-nee-uh-skohp-ee]: After numbing the eye, the eye doctor gently places a special lens on the surface to examine the area in the front of the eye that drains fluid.
Tonometry [toh-nom-i-tree]: Tonometry measures pressure in the eye. Medicine drops may be used to numb the eye.
Slit lamp: To find signs of eye inflammation, the eye doctor uses a special microscope called a slit lamp. It shines a light into one eye at a time so the doctor can look closely at the inside of the eye.
Fluorescein angiography [floo-res-ee-in an-jee-og-ruh-fee]: Doctors can find potential damage caused by some kinds of uveitis by injecting a substance that “lights up” the veins. This procedure provides a clear picture of the blood vessels in the retina at the back of the eye.
Optical coherence tomography (OCT): This non-invasive imaging test uses light waves to take cross-section pictures of your retina.
Laboratory tests: Laboratory tests may be done to rule out an infection or an autoimmune disorder.
How is Uveitis Treated?
The goal of treatment is to treat the inflammation and check the eyes regularly to help prevent damage and vision loss. Eye doctors treat uveitis to relieve pain, prevent vision loss from inflammation and complications of uveitis, and to treat the cause of the uveitis if known. It is important to follow the eye doctor’s instructions for treatment carefully throughout the duration of treatment as prescribed. Treatment of uveitis must continue as long as inflammation is active. It is not possible to know how long uveitis will last.
Treating Anterior Uveitis:
- Topical corticosteroids
- Eye drops to widen pupil
- Topical drop for elevated eye pressure
Treating Intermediate and Posterior Uveitis
- Antibiotics, antivirals, or other medications
- Corticosteroids – periocular injection, oral, intravenous, implant
- Nonsteroid anti-inflammatory drugs
- Immunosuppressive and biologic agents
- Corticotropin
Treatment of Uveitis
The goal of treatment is to treat the inflammation and check the eyes regularly to help prevent damage and vision loss. Eye doctors treat uveitis to relieve pain, prevent vision loss from inflammation and complications of uveitis, and to treat the cause of the uveitis if known. It is important to follow the eye doctor’s instructions for treatment carefully throughout the duration of treatment as prescribed. Treatment of uveitis must continue as long as inflammation is active. It is not possible to know how long uveitis will last. Possible treatments are:
Treating Anterior Uveitis
Topical corticosteroids [kawr-tuh-koh-ster-oid]: Eye doctors typically use topical corticosteroids in the form of eye drops or ointments to decrease inflammation as the first step except in cases where treatment of the underlying problem is the top priority. The strength of the medicine and how often it is needed will depend on the level of inflammation in the eye. If the uveitis does not respond to drops or ointments, the doctor may inject steroids next to the eye. Doctors will rarely prescribe steroid pills to treat anterior uveitis.
Eye drops to widen pupil: Vision loss from iritis can usually be prevented if diagnosed and treated. Eye doctors treat iritis with corticosteroid eye drops and eye drops that dilate (widen) the pupils. These eye drops can also help prevent the iris from “sticking” to the eye’s lens, a complication of anterior uveitis.
Topical drop for elevated eye pressure: If anterior uveitis causes increased pressure in the eye, the doctor may prescribe eye drops that help lower eye pressure to prevent damage to the optic nerve.
Treating Intermediate and Posterior Uveitis
Antibiotics, antivirals, or other medications: If the uveitis is caused by a bacterial, viral or fungal infection, then the treatment for that condition will involve anti-infective agents. It may be treated with or without corticosteroids.
Corticosteroids – periocular injection, oral, intravenous (IV): For non-infectious causes, the goal of therapy is to get the inflammation under control, quickly. This can be done by the use of corticosteroids. If the inflammation is in one eye only, the eye doctor may first try a steroid injection to the outside of the eyeball. If the eye does not respond or in the cases where both eyes are involved, the doctor will prescribe corticosteroid pills. If inflammation is very severe and/or the patient cannot take pills, the doctor will administer steroids through an IV route of administration. Side effects of corticosteroid use should be discussed with your eye care professional. Eye doctors know that the long-term use of corticosteroids may have serious side effects for patients (especially children), so a common goal of uveitis treatment is to slowly lower the dosage of steroids and then stop steroid treatment completely. Doctors work to bring the inflammation under control with the lowest amount of steroids needed.
Corticosteroids – implant: Many patients with chronic noninfectious posterior uveitis may benefit from a therapy involving a long-acting drug implant. The drug product is surgically implanted into the eye and is designed to release steroids directly into the back of the eye. This procedure seeks to reduce or eliminate many of the side effects common to oral corticosteroids.
Nonsteroid anti-inflammatory drugs: For some patients with chronic uveitis, eye doctors may prescribe nonsteroid anti-inflammatory drugs. These drugs can be an effective way to treat inflammation over a longer period of time. This treatment is not used very much.
Immunosuppressive and biologic agents: Even when the cause of uveitis is unknown, the uveitis may be related to problems with the body’s immune system. Autoimmune diseases are conditions in which parts of the body are attacked by the body’s own immune system. Immunosuppressive or cytotoxic drugs that weaken the body’s immune response have been effective in treating some kinds of uveitis. These drugs may be an option for some patients who have flare-ups of uveitis that affects both eyes, doesn’t respond well to corticosteroids or nonsteroidal anti-inflammatory drugs, or becomes severe enough to threaten vision. They can be swallowed as a pill, injected subcutaneously (under the skin), or infused into the blood within a vein. Taking immunosuppressant agents can make a person more vulnerable to infection. A small number of people with uveitis can benefit from treatment with a type of immunosuppressants known as biologics.
New treatments: A new treatment, corticotropin, is being examined. It is injected subcutaneously to reduce inflammation with less systemic side effects than steroids.
Vision Loss from Uveitis
Uveitis may cause blurry and reduced vision. When treated, vision may recover. In some cases, mostly in intermediate uveitis, posterior uveitis and panuveitis, where inflammation is recurrent and chronic, damage to the eye can occur, particularly to the retina and optic nerve, and cause permanent vision loss.
High eye pressure and glaucoma
Inflammation caused by uveitis can cause pressure in the eye to go up. This is called ocular hypertension. In addition, long-term steroid use may cause secondary glaucoma. The use of steroids can increase the amount of fluid produced by the ciliary body, causing the pressure inside the eye to rise. As many as one fifth of people with uveitis can develop ocular hypertension. Some of these individuals will develop glaucoma. The best way to prevent vision loss from glaucoma is by going to the eye doctor and following your treatment plan as directed.
Cataracts
Cataracts are a clouding of the eye’s lens. Eye doctors can remove the eye’s natural lens and replace it with a special artificial lens. However, if the cataracts are related to uveitis, eye doctors may not be able to perform surgery until the inflammation caused by uveitis is brought under control. In most cases, eye doctors want the eye to be free of inflammation for at least three months before performing cataract surgery. Sometimes, the artificial lens put in place by an eye doctor during cataract surgery can irritate the eye and cause anterior uveitis. In addition, long term use of corticosteroids for the treatment of uveitis can also increase the risk of developing cataracts.
Cystoid macular edema (CME)
This is a complication more commonly seen in intermediate uveitis, posterior uveitis, and panuveitis. CME is swelling of the macula which is the most sensitive part of the eye for vision needed for driving, reading and detailed work. If the swelling does not respond to treatment and is long standing, the sensitive cells under the fluid can eventually die. It can cause decreased vision which may lead to permanent vision loss.
Damage to the Vitreous
This is a complication seen in intermediate uveitis, posterior uveitis, and panuveitis. The vitreous is the clear gel-like substance that fills the eye. Rarely, inflammation from uveitis lets debris get into the vitreous. This may include blood and scar tissue. At first, this debris may cause floaters or flashes of light. If serious, it may block vision. Eye doctors will generally try medicines, and if the eye does not respond, the eye surgeon can remove the cloudy vitreous and replace it with a clear fluid. This procedure is called a vitrectromy.
Detached retina
This is a possible complication of posterior uveitis and panuveitis. Uveitis can increase the risk of developing a detached retina which will require immediate surgery to prevent blindness. As we age, the vitreous may shrink and pull away from the retina. This is called a vitreous detachment. Sometimes, the retina can pull off as the vitreous detaches. This is called a retinal detachment. Floaters or flashes of light may be signs of vitreous detachment or a retinal detachment.
Living with Uveitis
Modern treatments help control uveitis and can often prevent vision loss and blindness if the condition is found and treated early. Recovery depends on the type of uveitis and severity of inflammation. Uveitis can also come back. You must work with your eye care professional if you have uveitis. They know how to treat uveitis, but they have to work with you to find the best way to treat the condition. Stay informed, take your medicines as scheduled, and follow your treatment plan.
What You Do Makes a Difference
- Remember to take notes about how you feel. Write down your questions so you can make the most of your eye doctor visits.
- Explain to your eye doctor how the medicines you are taking affect you.
- Tell all of your other doctors about your eye medicines and all other drugs you’re taking.
- Tell the eye doctor about any changes in your physical condition, any changes in your medicine or any side effects.
- Call your eye doctor if you notice any unusual changes in your eyes, your vision or the way you feel in general.
- Schedule regular checkups and follow through with them.
- Take care of yourself! – your eyes and the rest of you along with them.
Follow Your Treatment Plan!
It’s up to you to follow your treatment plan and have follow-up visits as recommended by your eye doctor. Remember to report anything you believe may be a side effect of the medicine you are taking.
Don’t Skip Doses!
Skipping doses of your medicine may put your vision in danger and mislead your doctor. Be sure to tell your doctor if you’ve missed any doses.
After evaluating your progress, your doctor may try changing your doses, switching medicines or changing other parts of your treatment to find the best results for you.
Questions for Your Eye Doctor
You will have many questions as your doctor diagnoses and treats your uveitis. It’s helpful to keep a list of these questions, especially if they come to mind in between your doctor appointments. Write all your questions down and bring the list with you, then discuss them with your doctor. Here are some questions many people have:
- What do the medicines do?
- How much will they cost? Will my insurance help pay for them? (These may be questions for your insurance company, not your doctor).
- What are the possible side effects of my medicines?
- Can I do anything to lower the chance of side effects or reduce the effects?
- When exactly should I take my medicine? Can you please write down a detailed schedule?
- What should I do if I miss a dose?
- Do I need to do anything special to take care of my medicines?
Tips for Taking Your Medicine
- Learn about the medicines you are taking and the best way to use them. Find out whether they need special handling, such as storing them in the refrigerator.
- If you take a combination of drops and ointments, always apply the drops first.
- Schedule your doses around your normal routine, such as when you wake up, when you eat meals, and when you go to bed at night.
- Keep your medicines in plain sight. It’s easier to remember to take them.
- Keep medicines in a clean place. For example, if you carry them in your purse, put them in a sealed plastic bag to keep them clean.
- Take your medicines with you when you’re away from home. If you’re checking luggage at the airport, keep your medicines with you in your carry-on or in your purse.
- If you forget a dose, do not automatically double your next dose. Instead, follow your doctor’s instructions on what to do.
- If you can’t remember whether you took your medicines, simply use one dose at your next scheduled time.
You Have to Help Save Your Sight
Find support and encouragement from your family, friends and others. Sometimes it helps to talk to people who have experienced the same thing. It can help you to discuss side effects, share ways to remember your medicines and celebrate getting your uveitis under control.
Unfortunately, there are a few people who will lose vision despite commitment to working with their eye doctor and following their treatment plan. The future holds great promise for uveitis. New medicines and treatments continue to be developed. In the meantime, take heart in knowing that you’re doing everything possible to treat your condition. The doctor/patient team approach, support from others and promising scientific discoveries will help you look forward toward a bright future.
Resources for Eye Care
Prevent Blindness has a list of financial assistance resources for those in need of support in meeting their eye health needs and medications.